

To protect against potentially life-threatening consequences of leakage, some surgeons routinely use temporary diversion of the faecal stream from the anastomosis. In contrast, others use a selective approach in order to avoid the morbidity of a defunctioning stoma (DS) in all patients and defunction the anastomosis e.g. in case of adverse intra-operative events. However, a significant reduction of clinical leaks and need for urgent abdominal reoperation was observed after DS in a recent Swedish randomised multicenter trial, comparing outcome with and without DS in 234 patients after an uneventful low stapled anastomosis.
Based on these results, routine use of a DS in low anterior resections was recommended. Possible benefits of a routine DS need to be balanced against potential risks. A DS has considerable morbidity, an impact on quality of life as well as mortality related to stoma closure Thus, a selective use of DS may be justified, at least in the hands of surgeons who have ‘low’ CAL and CAL-(clinical anastomotic leak) related mortality rates.
A review and meta-analysis of recent literature were performed in order to appraise the incidence of CAL and the effect of a DS on the CAL rate after TME with very low anastomosis. A secondary endpoint was assessment of the leak-related mortality in the presence or absence of a DS. Finally, a sensitivity analysis was performed based on data from randomised trials in order to answer the question “In selective use of DS, what cut-off point calls for routine construction of DS in order to minimise patient risks?”. Data from randomised controlled trials and observational studies confirm that the presence of a defunctioning stoma significantly reduces the risk of a clinical leak as well as the reoperation rate for a leaking anastomosis. Thus, the evidence indicates that a defunctioning stoma should be constructed routinely at primary surgery. Leak-related mortality was not significantly different in patients with and without primary stoma in both study types. However, a 4.5 % mortality was observed in patients without primary stoma in randomised controlled trials versus 0% in patients with DS, while higher values were reported in observational studies for both groups of patients. Either way, a clinical leak must be timely diagnosed by close observation of all patients with colo-anal anastomosis. In the absence of a DS, the majority of these patients has to be treated by emergency secondary stoma construction and drainage. From a mortality risk point of view, the results of this review support routine construction of a protective stoma at TME. However, a selective use of DS at TME may be justified for some surgical teams, on the condition that the overall leak- and stoma closure-related mortality does not exceed 0.9 %.
Thus, each team should audit its leak rate, leak-related and stoma closure-related mortality rates. A DS can be used selectively in complex procedures, in case of intraoperative difficulty, in patients with poor general condition or in those who have to start chemotherapy within a short delay.
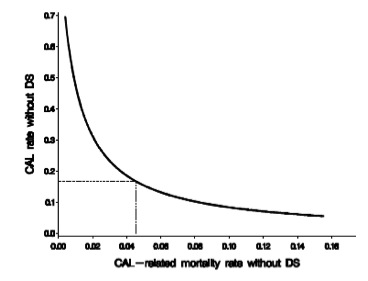
Figure 1. Relation between clinical anastomotic leak (CAL) rates without defunctioning stoma (DS) for a range of possible CAL-related mortality rates without DS leading to an overall mortality of 0.9%, including a given mortality due to stoma closure of 0.9%. The dotted lines denote the specific situation based on the CAL-related mortality of 4.55% in patients without a primary DS in randomised studies, corresponding with an ‘allowed’ CAL rate without DS of 16.6%.
Reference
Mortality risk analysis following routine vs selective defunctioning stoma formation after total mesorectal excision for rectal cancer Pata G, D’Hoore A, Fieuws S, Penninckx F. Colorectal Dis. 2009 Oct;11(8):797-805. Epub 2008 Oct 1. Review.